Given team 403's objective is to improve the efficiency and optimization of the infusion chairs and their connecting processes to maximize the number of patients to be seen and treated, it is imperative to identify issues that contribute to the high turnaround time for pharmacy processing. Some of the factors that contribute to the inefficiency of their current process are scheduling issues with patients, communication issues between TMH forecasting process and external referrals, inefficiencies between the doctor and infusion unit, performance bottleneck in scheduling patients, and significant variability in operation procedures. These and more known issues are listed in more detail below:
- The unit doesn’t get to see patient until after the patient sees the doctor.
- -Process: Patient arrives in the morning, sees the Doctor, may need to do lab work, then gets treatment (potential root cause of why 8am to 10am utilization is low)
- Some regimens need a chair for 8 hours.
- There is no space to add on new types of treatments.
- -Therefore, cancellation of appointments occur.
- There can be holds on schedules for potential blood requirements of patients.
- There can be back to back scheduling of pateints which will create bottlenecks.
- The patient timing is dependent on the doctor and if the patient is on time.
- New patient scheduling issues:
- -Need "Intent to Treat" athorization which can take 4-5 days.
- -The cancer center scheduling office is notified last minute as the scheduling systems do not communicate.
- Sompe patients need pre-procedures done before infusions and due to poor communication, the pre-treatments have not beeen done.
- -Pateint has to reschedule appointment.
- When a patient needs radiation or chemotherapy:
- -Before radiation, the patient must recieve chemotherapy. These treatments areas are on different floors.
- -Radiation and chemotherapy software systems do not communicate well.
- -Nurse navigators schedule and coordinate these two types of treatments.
- Patient education is conducted by nurse navigators in advance of chemitherapy treatments.
- -Last minute appointments also must go through the hour long patient education.
A patient processing diagram was created to visually represent the flow of the patient through the Cancer Center:
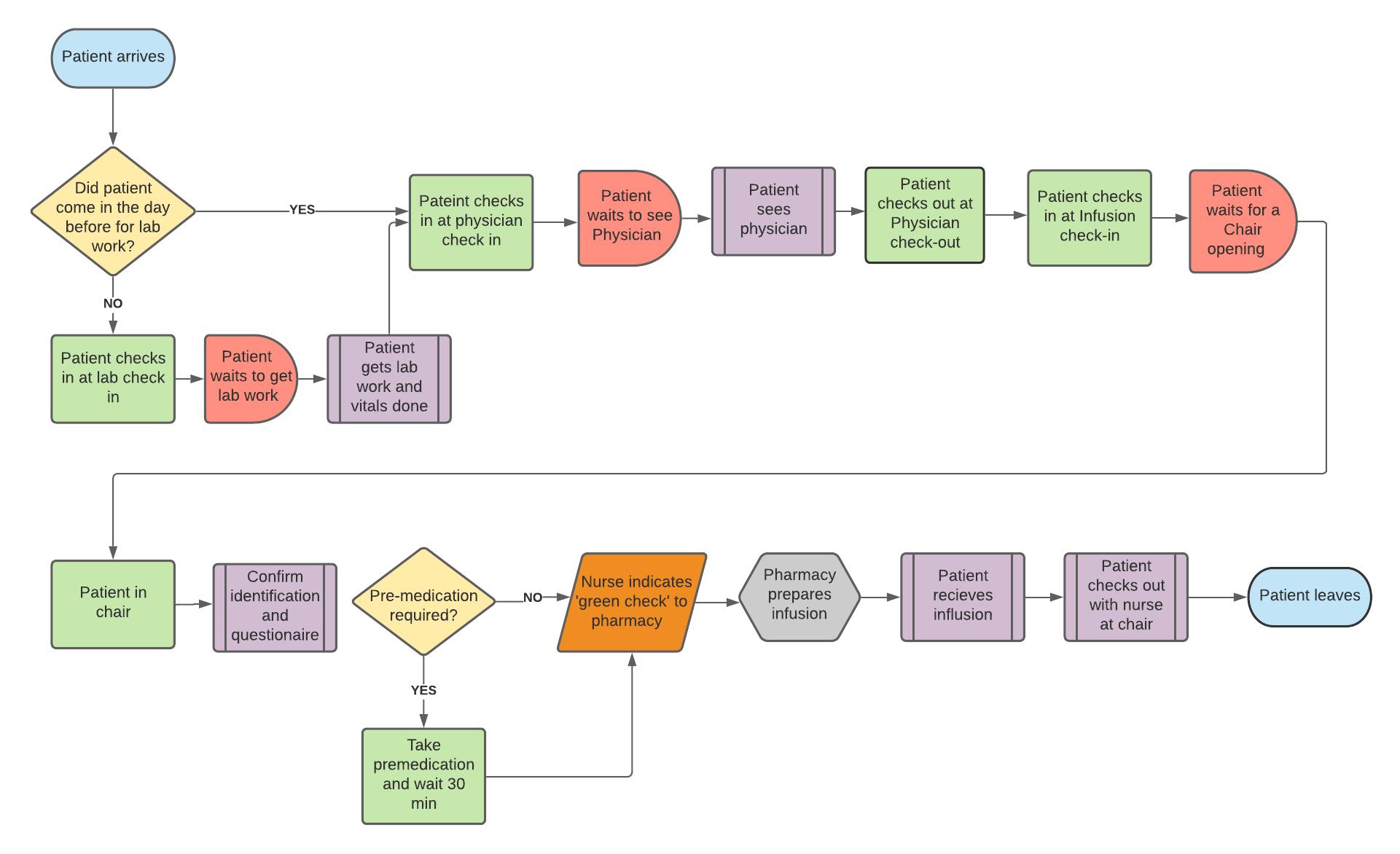
Figure 2: Patient Process Map